

Medication does not cure depression, and understanding that distinction matters more than most people realize. The role of medication in depression treatment is to reduce the severity of symptoms enough that you can engage with the real work of recovery. Think of it as stabilizing the ground beneath your feet so therapy, lifestyle changes, and support systems can actually take hold. With appropriate treatment, 70 to 80% of people with major depressive disorder experience significant symptom reduction. That is a meaningful number, but it only holds when medication is used correctly and in context.
Table of Contents
- Key takeaways
- How medication works in the depressed brain
- Types of antidepressants and what sets them apart
- Managing side effects without giving up on treatment
- Why medication alone is not enough
- My honest take on medication and realistic expectations
- AI tools that support your depression treatment
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Medication reduces symptoms, not causes | Antidepressants stabilize brain chemistry to make other treatments more effective, not to fix depression permanently. |
| Effects take time to appear | Most antidepressants require 7 to 14 days of consistent use before you notice any change in mood. |
| Side effects are common but manageable | 82.9% of patients report at least one side effect, but most can be addressed through dose adjustments or medication changes. |
| Medication works best alongside therapy | Combining medication with therapy produces faster improvement and lower relapse rates than either treatment alone. |
| Finding the right med takes trial | Medication selection is an iterative process requiring close monitoring and honest communication with your provider. |
How medication works in the depressed brain
To understand what antidepressants actually do, you need a basic picture of what depression does to the brain. Depression is not simply a shortage of serotonin. That explanation has been popular for decades, but it is an oversimplification. What actually happens is more complex and, in some ways, more interesting.
Depression disrupts the communication between neurons. Neurotransmitters like serotonin, norepinephrine, and dopamine carry signals across the gaps between nerve cells. In depression, these signals become weaker, less frequent, or get absorbed back too quickly before they can do their job. Most antidepressants work by slowing that reabsorption process, a mechanism called reuptake inhibition. This keeps more of the neurotransmitter available in the synapse, giving signals a better chance of getting through.
But there is a more important effect that often gets overlooked. Antidepressants support neuroplasticity, the brain’s ability to form new connections and strengthen existing pathways. This is why the medication effects on depression go beyond simply “balancing chemicals.” The medication creates conditions in which your brain can actually rewire itself. That rewiring is what makes therapy stick, what makes new coping habits form, and what makes recovery sustainable.
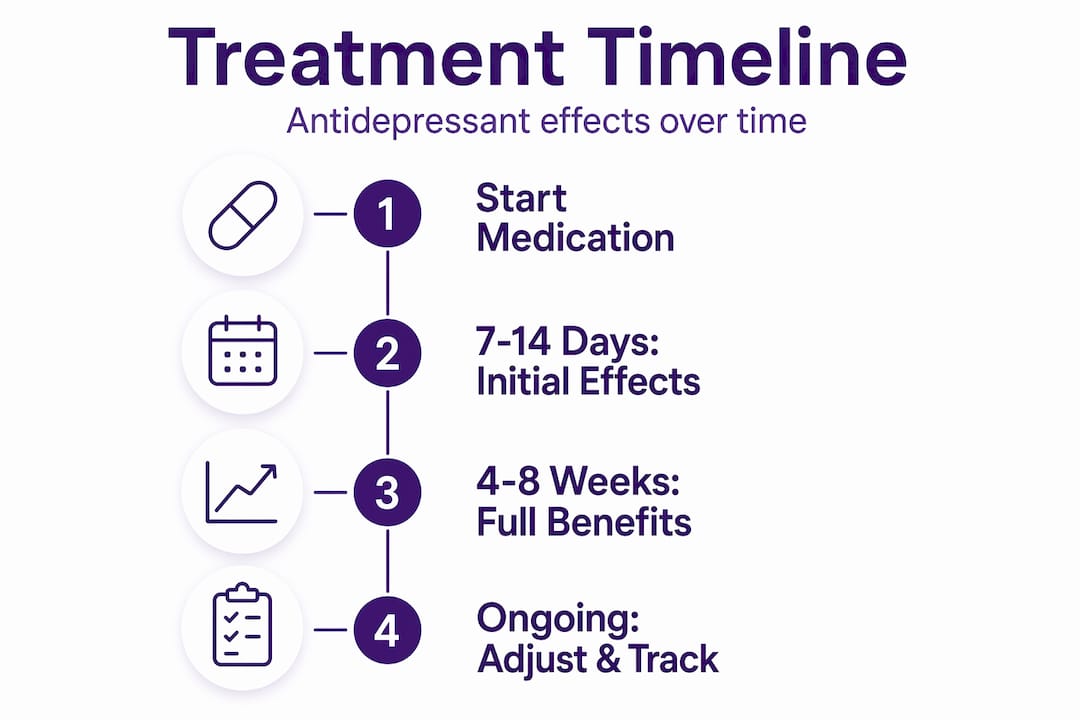
This also explains the timeline. Initial effects appear after 7 to 14 days of consistent use, but the full neurological benefit often takes 4 to 6 weeks. Stopping early because you “don’t feel different yet” is one of the most common reasons medication fails. Adherence during that window is not optional. It is the whole point.
Pro Tip: Set a recurring phone reminder for your medication at the same time each day. Consistent dosing matters more than most people expect, especially in the first 6 weeks.
One honest limitation worth naming: antidepressants treat symptoms. They do not resolve the underlying causes of depression, whether those are trauma, chronic stress, relationship problems, or thought patterns. That is the work of therapy and lived change. Medication gives you the neurological stability to do that work.
Types of antidepressants and what sets them apart
Not all antidepressants work the same way, and the differences matter when your doctor is choosing what to prescribe. Here is a practical overview of the main classes.
| Class | How it works | Common examples | Typical use case |
|---|---|---|---|
| SSRIs | Block serotonin reuptake | Fluoxetine, sertraline, escitalopram | First-line treatment for most depression types |
| SNRIs | Block serotonin and norepinephrine reuptake | Venlafaxine, duloxetine | Depression with anxiety or chronic pain |
| TCAs | Block multiple neurotransmitter reuptakes | Amitriptyline, nortriptyline | Severe depression, often when SSRIs fail |
| MAOIs | Block breakdown of neurotransmitters | Phenelzine, tranylcypromine | Treatment-resistant or atypical depression |
| Atypical | Varied mechanisms | Bupropion, mirtazapine | When SSRIs cause intolerable side effects |
SSRIs are almost always the starting point. They have the most research behind them, a relatively tolerant side effect profile, and decades of clinical use. SNRIs are often chosen when anxiety is a significant part of the picture or when chronic pain is present alongside depression.
TCAs and MAOIs are older classes. They work, sometimes very well, but their side effect profiles are more demanding. MAOIs in particular require dietary restrictions to avoid dangerous interactions with tyramine-containing foods. These are not first choices, but they remain relevant for people who have not responded to newer medications.
The most significant recent development in the antidepressants and treatment space is esketamine for treatment-resistant depression. Unlike traditional antidepressants that can take weeks to work, esketamine can produce relief within hours. It is administered as a nasal spray in a clinical setting and is approved specifically for people who have not responded to at least two other antidepressants.
A few other points worth knowing:
- Atypical antidepressants like bupropion are often chosen when sexual side effects from SSRIs are a problem.
- Mirtazapine is sometimes used when sleep disruption and appetite loss are severe symptoms.
- Treatment duration typically runs at least 6 months after symptoms improve, not just until you feel better.
- Your provider may adjust your treatment plan multiple times before finding what works best for you.
Managing side effects without giving up on treatment
82.9% of people on antidepressants report at least one side effect. That statistic sounds alarming, but context matters. Most side effects are mild, appear in the first few weeks, and often resolve on their own as your body adjusts. The ones that persist are usually manageable with the right support.
The most commonly reported side effects include:
- Weight gain (reported by 64% of patients)
- Nausea or vomiting (51%)
- Dry mouth (49%)
- Headache (41%)
- Sexual dysfunction (varies widely by medication class)
Not everyone experiences all of these, and severity varies significantly. Certain factors increase risk, including being female, having low physical activity levels, unemployment, low income, and longer duration of medication use. This is not about blame. It is about understanding that side effects are not random. They follow patterns, and knowing your risk profile helps you have a more productive conversation with your provider.
The most damaging thing you can do when side effects appear is stop your medication abruptly. Abrupt discontinuation causes withdrawal symptoms including dizziness, irritability, and flu-like feelings. If you need to stop, your provider will guide you through a gradual taper over weeks or months.
Pro Tip: Keep a simple daily log of your mood, energy, and any physical symptoms. Bringing this to your provider appointments turns vague impressions into useful data that actually speeds up the adjustment process.
The iterative process of medication management means your first prescription may not be your final one. Dose adjustments, switches to a different class, or adding a second medication are all normal parts of treatment. Persistence through this process, with good communication, is what separates people who find relief from those who give up too early.

Why medication alone is not enough
Medication stabilizes your brain. It does not teach you how to think differently, process grief, rebuild relationships, or develop the habits that protect against relapse. That is the honest truth about how medication helps depression, and it is not a criticism of medication. It is a description of what it is actually designed to do.
Here is a practical framework for thinking about integrated treatment:
- Medication reduces the biological intensity of depression, making it possible to function and engage with other treatments.
- Therapy (particularly cognitive behavioral therapy or CBT) addresses the thought patterns, emotional responses, and behavioral habits that maintain depression.
- Exercise has demonstrated antidepressant effects in its own right, improving mood through endorphin release and reducing inflammation.
- Sleep hygiene is not optional. Disrupted sleep worsens every symptom of depression and reduces medication effectiveness.
- Nutrition and social connection provide the daily inputs that either support or undermine recovery.
Combining medication with therapy produces faster symptom improvement, lower relapse rates, and better overall outcomes than either approach alone. This is not a soft claim. It is one of the most replicated findings in depression research.
“Successful care requires an ongoing therapeutic relationship with iterative communication to adjust treatment based on mood and side effects.” — Blue Sky Psychiatry on integrated depression care
For moderate to severe depression, medication is often necessary to reach the baseline stability where therapy can be effective. You cannot do the cognitive work of CBT when your brain is in crisis mode. Medication lowers the volume enough that you can hear the lesson. Exploring holistic depression treatment strategies alongside your medication plan gives you the fullest picture of what recovery can look like.
The healthy coping skills you build during treatment, with the support of both medication and therapy, are what carry you through once medication is eventually reduced or stopped. That is the actual goal: not lifelong medication dependence, but the skills and neurological health to sustain recovery on your own terms.
My honest take on medication and realistic expectations
I have spent years reading the research and talking with people navigating depression treatment, and the single most common mistake I see is expecting medication to do everything. People start a prescription, wait two weeks, feel “not that different,” and conclude it is not working. Then they stop.
What I have learned is that the trial-and-error nature of antidepressant treatment is not a flaw in the system. It reflects genuine biological individuality. Your neurotransmitter profile, your metabolism, your history with stress and trauma, all of it shapes how you respond to a given medication. The medication selection process is not guesswork. It is calibration.
What I find most underappreciated is the neuroplasticity angle. When medication is working, it is not making you feel artificially happy. It is creating the biological conditions for your brain to change. That change requires input. It requires therapy, movement, sleep, and honest reflection. Medication opens the door. You still have to walk through it.
My take: be patient with the timeline, be honest with your provider about side effects, and resist the urge to judge medication by how you feel in week two. The people who see the best outcomes are not the ones who found the perfect drug immediately. They are the ones who stayed engaged with the process.
— dushyantha
AI tools that support your depression treatment
Medication and therapy are the foundation, but the space between appointments is where a lot of people struggle. Cognicareai offers a directory of AI-powered mental health tools designed to fill that gap, from mood tracking apps to AI-guided mindfulness and personalized self-care programs. These tools do not replace your provider or your prescription. They help you stay consistent, monitor your symptoms between visits, and build the daily habits that make treatment more effective. If you are looking for ways to strengthen your recovery beyond what happens in the clinic, exploring what AI is doing for mental health care is a practical next step.
FAQ
How long does it take for antidepressants to work?
Most antidepressants require 7 to 14 days of consistent use before initial effects appear, with full benefits often taking 4 to 6 weeks. Stopping early is one of the most common reasons treatment fails.
Can medication alone treat depression?
Medication reduces biological symptoms but does not address the underlying causes of depression. Research consistently shows that combining medication with therapy produces better and more lasting outcomes than medication alone.
What are the most common antidepressant side effects?
The most frequently reported side effects include weight gain, nausea, dry mouth, and headache, with studies showing 82.9% of patients experience at least one. Most are manageable and often improve within the first few weeks.
Is it safe to stop taking antidepressants suddenly?
No. Stopping antidepressants abruptly can cause withdrawal symptoms including dizziness, irritability, and flu-like sensations. Always work with your provider to taper gradually over weeks or months.
What if the first antidepressant does not work?
This is common and expected. Finding the right medication and dose is an iterative process, and switching classes or adjusting dosage is a normal part of treatment, not a sign that medication cannot help you.