

Treatment-resistant depression (TRD) is defined as major depression that fails to respond adequately after at least two antidepressant treatments given at the right dose and for the right duration. Approximately 30% of individuals with major depressive disorder meet the clinical criteria for TRD. That figure means millions of people are not failing their treatment. Their treatment is failing them. TRD reflects the biological diversity of depression rather than any personal shortcoming, and effective options exist. Understanding what is treatment-resistant depression is the first step toward finding a path forward.
What causes treatment-resistant depression?
Depression is not a single disease. It is a cluster of conditions with different biological roots, and that diversity is the primary reason some people do not respond to standard antidepressants. Researchers now recognize that neuroinflammation and oxidative stress play a direct role in TRD. People with an inflammatory subtype of major depressive disorder show elevated biomarkers such as C-reactive protein (CRP) and interleukin-6, both of which correlate with poor antidepressant response. That means a standard SSRI may simply be targeting the wrong biological mechanism.
Sex-based biology adds another layer of complexity. Sex-based differences influence how TRD develops and how people respond to treatment, which is why personalized care plans matter far more than one-size-fits-all protocols. Hormonal fluctuations, immune system differences, and metabolic variation all shape how a person’s brain responds to medication.

Psychosocial and medical factors compound the picture significantly. Untreated chronic pain, cardiovascular disease, and autoimmune conditions all interfere with antidepressant effectiveness. Trauma history, social isolation, and ongoing stressors can sustain depressive symptoms regardless of what medication a person takes. Exploring the complexity of depression’s many faces helps explain why no single drug works for everyone.
A critical and often overlooked factor is pseudo-resistance. Undiagnosed sleep apnea, thyroid dysfunction, or poor medication adherence can mimic true TRD. Before a clinician labels a case as treatment-resistant, ruling out these reversible causes is a required first step.
- Neuroinflammation: Elevated CRP and interleukin-6 reduce antidepressant effectiveness in a measurable inflammatory subtype.
- Biological heterogeneity: Depression involves multiple distinct biological pathways, not one uniform disease process.
- Sex-based variation: Hormonal and immune differences between sexes affect both TRD risk and treatment response.
- Medical comorbidities: Thyroid disorders, sleep apnea, and chronic pain frequently sustain depressive symptoms.
- Psychosocial stressors: Trauma, poverty, and social isolation maintain depression independently of brain chemistry.
- Pseudo-resistance: Nonadherence or undiagnosed medical conditions can look exactly like true TRD.
Pro Tip: Before accepting a TRD diagnosis, ask your doctor to run a full metabolic panel and thyroid screen. Correcting an undiagnosed thyroid condition has resolved apparent treatment resistance in many cases.
How is treatment-resistant depression diagnosed?
The current clinical definition of TRD requires failure to respond to at least two antidepressant trials, each at an adequate dose and for an adequate duration, typically six to eight weeks. That standard comes from major clinical bodies and shapes how insurers and providers authorize advanced treatments. A detailed treatment history including drug names, doses, duration, and side effects is not optional. It is the foundation of any accurate TRD diagnosis and a requirement for approving advanced interventions.
A newer framework is gaining ground in clinical practice. The “Difficult-to-Treat Depression” (DTD) model moves beyond counting failed medication trials. It considers the full longitudinal course of illness, functional impairment, and psychosocial stressors. The table below shows how TRD and DTD differ in practice.
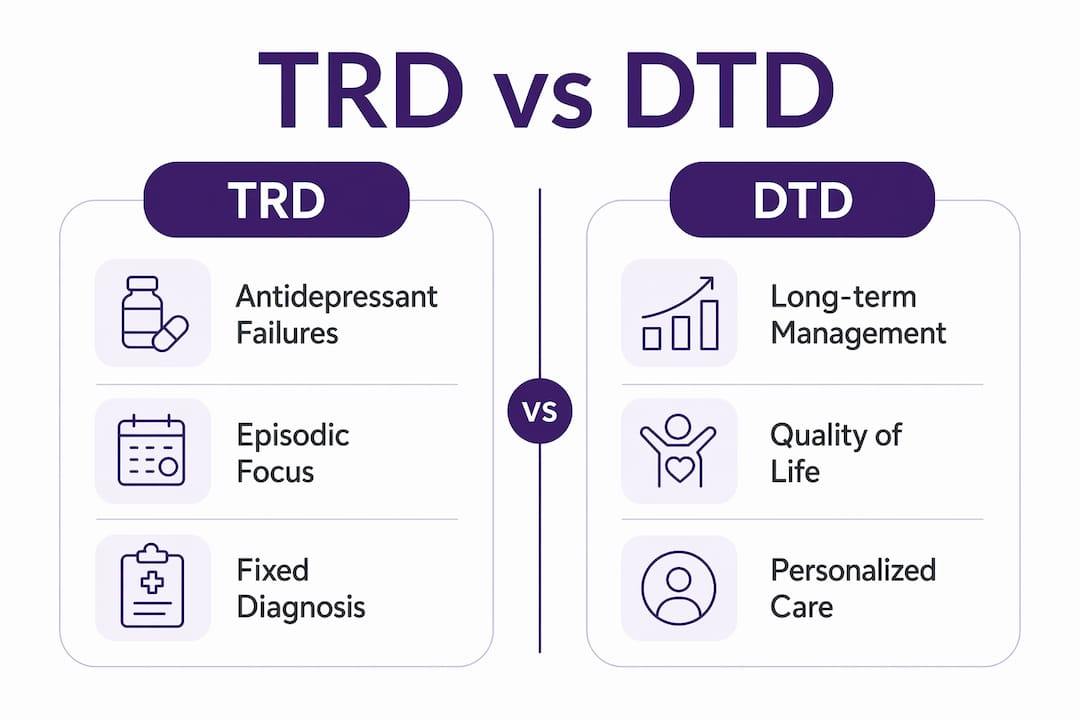
| Feature | Treatment-Resistant Depression (TRD) | Difficult-to-Treat Depression (DTD) |
|---|---|---|
| Core definition | Two failed adequate antidepressant trials | Persistent impairment across the illness course |
| Time frame | Episodic, trial-by-trial | Longitudinal, ongoing |
| Focus | Medication response | Functional outcomes and quality of life |
| Comorbidities | May be noted but not central | Central to assessment and planning |
| Framework origin | Pharmacological research | Clinical and psychosocial integration |
The DTD framework matters because it shifts focus from episodic treatment failures to long-term illness management. A person may have responded partially to medication but still live with significant disability. DTD captures that reality where TRD does not. Both frameworks agree on one thing: comprehensive assessment must include functional impairment, comorbid conditions, and the full patient history.
What are the treatment options for resistant depression?
Treatment options for TRD have expanded considerably by 2026. The goal is no longer simply to try another antidepressant. Next-step treatments now prioritize augmentation strategies, neuromodulation, and newer pharmacological agents. An integrated treatment approach combining psychotherapy, medication, and neuromodulation consistently outperforms sequential medication trials alone.
Pharmacological options
- Augmentation: Adding a second-generation antipsychotic such as aripiprazole or quetiapine to an existing antidepressant is a common and well-studied first move.
- Antidepressant switching: Moving to a different class, such as from an SSRI to an SNRI or a tricyclic, targets different neurotransmitter systems.
- Ketamine and esketamine: Ketamine works through the glutamate system rather than serotonin, producing rapid antidepressant effects within hours. The FDA-approved nasal spray esketamine (Spravato) is now a standard option for TRD. Reviewing the role of medication in depression clarifies how these newer agents fit into a broader treatment plan.
Neuromodulation therapies
FDA-approved neuromodulation treatments for TRD include repetitive Transcranial Magnetic Stimulation (rTMS), Electroconvulsive Therapy (ECT), and Vagus Nerve Stimulation (VNS). Each works by directly modulating brain activity rather than altering neurotransmitter levels through medication.
- rTMS: Uses magnetic pulses to stimulate specific brain regions. Non-invasive, performed outpatient, and approved for TRD.
- ECT: The most effective treatment for severe TRD. Modern ECT is performed under anesthesia and carries far fewer risks than its historical reputation suggests.
- VNS: A surgically implanted device that stimulates the vagus nerve. Approved for chronic, recurrent TRD unresponsive to other treatments.
Emerging therapies
Psychedelic-assisted therapy, including psilocybin-assisted psychotherapy, is under active clinical investigation as of 2026. Early trial data show meaningful antidepressant effects in treatment-resistant populations. These treatments are not yet widely available outside clinical trials, but they represent a genuine frontier in TRD care.
Pro Tip: When discussing neuromodulation with your psychiatrist, ask specifically about accelerated TMS protocols. Some clinics now offer compressed treatment schedules that deliver results in days rather than weeks.
How can you cope with treatment-resistant depression?
Medical treatment is the foundation, but daily coping strategies directly affect outcomes. The following steps work alongside clinical care, not instead of it.
- Exercise consistently. Aerobic exercise at moderate intensity, performed at least three times per week, produces measurable antidepressant effects. It is not a cure, but it reliably reduces symptom severity.
- Prioritize sleep hygiene. Disrupted sleep worsens depressive symptoms and reduces medication effectiveness. A fixed sleep schedule, a dark room, and limiting screens before bed are concrete starting points.
- Eat to support brain health. Anti-inflammatory diets rich in omega-3 fatty acids, leafy greens, and whole grains align with what research knows about neuroinflammation and mood. Holistic depression treatment strategies detail how nutrition fits into a broader plan.
- Engage in structured psychotherapy. Cognitive Behavioral Therapy (CBT) and Acceptance and Commitment Therapy (ACT) build coping skills that medication cannot provide. Therapy also addresses the trauma and psychosocial stressors that sustain TRD.
- Join a peer support group. Connecting with others who share similar experiences reduces isolation and provides practical strategies from people living with the same challenges.
- Advocate clearly with your provider. Bring a written list of every medication you have tried, the doses, how long you took it, and what happened. A detailed treatment timeline is the single most useful document you can bring to a psychiatric appointment.
- Use digital mental health tools as adjunct support. AI-powered apps, mindfulness programs, and therapy chatbots offer between-session support. Personalizing mental health care with AI has become a practical option for people managing complex depression.
- Manage social stressors actively. Financial stress, relationship conflict, and work pressure sustain depression. Addressing these through counseling, social services, or community resources is part of treatment, not separate from it.
Lifestyle and psychosocial interventions including exercise, nutrition, sleep hygiene, and mindfulness are proven to improve coping and overall well-being alongside medical treatments. They are not optional extras. They are part of the treatment plan.
Key Takeaways
Treatment-resistant depression is a biologically complex condition requiring personalized, integrated care that goes well beyond sequential antidepressant trials.
| Point | Details |
|---|---|
| Clinical definition of TRD | Two failed antidepressant trials at adequate dose and duration define treatment-resistant depression. |
| Prevalence | Approximately 30% of people with major depressive disorder meet TRD criteria. |
| Biological causes | Neuroinflammation, oxidative stress, and biological heterogeneity drive resistance, not patient failure. |
| Expanded treatment options | FDA-approved options include esketamine, rTMS, ECT, and VNS alongside augmentation strategies. |
| Coping alongside treatment | Exercise, sleep hygiene, psychotherapy, and digital tools measurably improve outcomes in TRD. |
Why the “resistant” label may be holding you back
The word “resistant” implies a fixed state. That framing is clinically inaccurate and personally harmful. Depression that has not responded to two medications is not permanent. It is a signal that the treatment approach needs to change, not that the person is beyond help.
What I have seen consistently is that people who shift from a passive “nothing works for me” stance to an active partnership with their care team get better outcomes. That means asking hard questions, requesting specific tests, pushing for neuromodulation referrals when medication has failed, and tracking symptoms between appointments. The DTD framework supports this shift. It treats depression as an ongoing condition to manage rather than a series of failed drug trials to survive.
The integrated model, combining early psychotherapy with medication and neuromodulation rather than waiting for each to fail before trying the next, is where the field is moving. Clinicians who still practice strict sequential trials are working from an older playbook. You have every right to ask your provider about combining approaches from the start.
New treatments like esketamine and accelerated rTMS have changed what is possible for people with resistant depression. The pipeline for 2026 and beyond, including psilocybin-assisted therapy, is genuinely promising. Persistence, specificity, and an integrated care team are the three factors that most consistently predict improvement.
— dushyantha
AI-powered tools that support depression management
Managing persistent depression requires support between clinical appointments. Cognicareai offers a curated directory of AI-powered mental health tools designed to complement your existing treatment plan, not replace it.
From mindfulness apps to therapy chatbots and personalized self-care programs, Cognicareai connects you with resources that adapt to your specific needs. These tools provide structured support during the hours when your therapist or psychiatrist is unavailable. People managing complex depression benefit from consistent, low-barrier access to coping resources, and AI-powered tools deliver exactly that. Visit Cognicareai to find the right tools for where you are right now.
FAQ
What is treatment-resistant depression, exactly?
Treatment-resistant depression is major depressive disorder that does not improve adequately after at least two antidepressant treatments given at the correct dose and for a sufficient duration, typically six to eight weeks each.
What are the signs of treatment-resistant depression?
The primary sign is persistent depressive symptoms, including low mood, fatigue, and loss of interest, despite completing multiple adequate antidepressant courses. Functional impairment that continues across treatments is a key indicator.
Can depression really be treatment-resistant?
Yes. Approximately 30% of people with major depressive disorder meet clinical criteria for TRD. Biological factors including neuroinflammation and genetic variation in drug metabolism explain why standard antidepressants fail for a significant portion of patients.
What medications work for treatment-resistant depression?
FDA-approved pharmacological options include esketamine (Spravato) and augmentation with second-generation antipsychotics such as aripiprazole. Ketamine infusions are also widely used off-label for rapid symptom relief.
Is treatment-resistant depression permanent?
No. TRD is not a permanent state. Neuromodulation therapies like ECT and rTMS, newer agents like esketamine, and integrated treatment approaches combining psychotherapy with medication produce meaningful improvement in the majority of people who pursue them.