

The role of chatbot architecture in therapy apps is far more consequential than most developers and clinicians realize. Most people assume the quality of a therapy chatbot depends primarily on which AI model powers it. That assumption is wrong, and the evidence is striking. A cognitive layer architecture has been shown to outperform both standalone large language models and human clinicians on key CBT competencies. Architecture, not just model choice, determines whether a therapy app genuinely helps users or inadvertently harms them.
Table of Contents
- Key takeaways
- The role of chatbot architecture in therapy apps
- Clinical effectiveness and safety in chatbot design
- Trauma-informed care principles in chatbot design
- Practical guidelines for professionals and developers
- Future trends and challenges in therapy chatbot architecture
- My perspective on what architecture really means for therapy apps
- How Cognicareai supports smarter therapy chatbot development
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Architecture drives outcomes | Specialized cognitive layers outperform general LLMs and even human clinicians on measurable CBT competencies. |
| Modular design improves safety | Separating conversation, assessment, intervention, and crisis modules creates more controllable and safer therapy systems. |
| Trauma-informed design matters | Embedding SAMHSA’s trauma-informed care principles into chatbot architecture reduces re-traumatization risk for vulnerable users. |
| Regulatory pressure is growing | FDA advisory discussions now target generative AI mental health tools, making architecture compliance a legal and clinical concern. |
| Clinicians and developers must collaborate | Effective therapy chatbot design requires ongoing input from both clinical practitioners and technical architects. |
The role of chatbot architecture in therapy apps
When clinicians and developers talk about therapy app chatbots, the conversation usually gravitates toward which model is being used. GPT-4o, Claude, Gemini. The model matters, but it is only one layer of a much more complex system. The term “chatbot architecture” refers to the full technical and clinical structure of how a conversational AI system is designed, organized, and constrained to serve a therapeutic purpose. Think of it as the difference between a car engine and the entire vehicle. The engine matters, but without brakes, a steering wheel, and safety belts, it is dangerous.
LLM-based mental health chatbots predominantly use decoder-only or encoder-decoder generative architectures for counseling contexts, favoring flexible conversational output over the more rigid encoder-only models. This architectural preference reflects a clinical reality: therapy requires nuanced, context-sensitive dialogue, not just text classification.
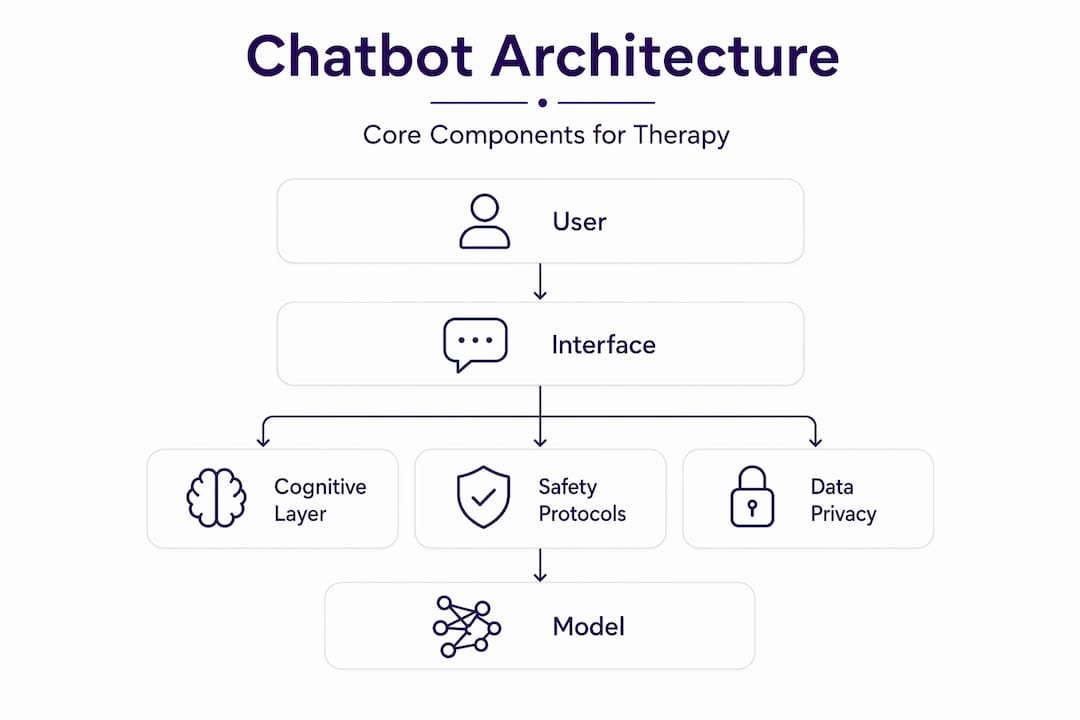
The core components of a well-designed therapy chatbot architecture include:
- Generative language model layer: The conversational engine, typically a decoder-only or encoder-decoder model, responsible for producing natural, empathic responses.
- Cognitive or therapeutic reasoning layer: A structured overlay that constrains and guides the model’s outputs according to evidence-based frameworks like CBT or DBT.
- Assessment module: Standardized clinical tools such as PHQ-9 for depression and GAD-7 for anxiety, integrated to track user progress over time.
- Intervention module: Structured therapeutic tasks, psychoeducation prompts, and coping exercises delivered at appropriate moments in the conversation.
- Crisis detection and escalation module: Automated detection of high-risk language with immediate routing to emergency resources or human clinicians.
- Security and compliance layer: Data encryption, HIPAA-relevant access controls, and audit logging across frontend, backend, and database components.
One real-world example comes from a GPT-4o therapy platform that integrated all of these layers with multilingual support, demonstrating that modular design is both technically feasible and clinically meaningful.
Pro Tip: When evaluating a therapy chatbot platform, ask for a system architecture diagram. If the vendor cannot show you how crisis escalation, assessment, and conversation modules are separated and monitored, treat that as a significant red flag.
Clinical effectiveness and safety in chatbot design
Here is where the evidence gets genuinely surprising. A randomized, double-blind trial with 227 participants, later validated against 19,674 real-world transcripts from 8,920 users, found that a cognitive layer architecture outperformed both standalone LLMs and human clinicians on key CBT competencies. The cognitive layer operationalizes therapeutic reasoning. It does not allow the model to improvise freely. That constraint is a feature, not a limitation.
Safety is where architectural choices carry the most clinical weight. The critical safety features that architecture must support include:
- Human-in-the-loop escalation: Flexible LLM systems require more robust emergency protocols than rule-based bots because their outputs are less predictable.
- Emergency alerting: Automated detection of suicidal ideation or crisis language with immediate, structured response pathways.
- Session monitoring and audit trails: Logged conversations that supervisors or clinicians can review for quality assurance.
- Boundary enforcement: Architectural constraints that prevent the chatbot from diagnosing, prescribing, or making clinical determinations beyond its defined scope.
The risks of poor architecture are not theoretical. NAM’s panel discussions on AI chatbots in mental health specifically identified over-reliance, pseudo-relationships, and social withdrawal as outcomes linked to modifiable design factors. The architecture either builds in safeguards or it does not.
“Non-judgmental mirroring and 24/7 availability improve comfort but heighten the need for safety limits and AI literacy to prevent harmful user dependence.” — NAM, 2026
A substance use disorder pilot using an AI-powered coaching chatbot demonstrated usability success but explicitly flagged the need for additional safety infrastructure. The lesson is consistent across studies: the more flexible the underlying model, the more structured the safety architecture must be to compensate.
Trauma-informed care principles in chatbot design
Trauma-informed care (TIC) is not a soft add-on for therapy apps. It is a clinical framework that, when absent from chatbot architecture, creates measurable harm risk for vulnerable users. SAMHSA’s TIC model identifies six core principles that must translate directly into design decisions.
- Safety: The chatbot interface, tone, and dialogue management must never feel threatening or coercive. This means avoiding confrontational prompting and building in user control over session pacing.
- Trustworthiness and transparency: Users must understand they are interacting with an AI. Architecture should enforce clear non-human disclosure at session start and whenever the topic escalates.
- Peer support: Where possible, design pathways that connect users to peer communities or human support networks rather than positioning the chatbot as a sole resource.
- Collaboration and mutuality: Dialogue management should give users meaningful choices about conversation direction rather than forcing scripted paths.
- Empowerment and choice: The chatbot should reinforce user agency. Architectural features like session summaries, progress tracking, and goal-setting tools operationalize this principle.
- Cultural, historical, and gender sensitivity: Language models must be fine-tuned or constrained to avoid culturally biased responses. Multilingual support and culturally adapted content are architectural requirements, not optional features.
A scoping review of 38 publications evaluating 28 mental health conversational agents found that most existing platforms fell short on TIC compliance, particularly around transparency and cultural sensitivity. For developers building or updating a therapy chatbot, this review is required reading. Integrating trauma-informed design frameworks into architecture from the start is significantly easier than retrofitting them after deployment.
Practical guidelines for professionals and developers

Choosing or building a therapy chatbot architecture is not a purely technical decision. It is a clinical one. Whether you are a mental health professional evaluating a platform or a developer designing one, these principles should guide your process.
The most common mistake is selecting a general-purpose LLM and wrapping it in a mental health-themed interface. A general-purpose LLM alone is insufficient for therapy quality. Specialized cognitive layers deliver measurable improvements in clinical competencies and outcomes. The architecture must embed therapeutic reasoning, not just enable conversation.
Practical guidelines for both audiences:
- Demand modularity: Separate modules for conversation, assessment, intervention, and crisis management allow for independent monitoring, updating, and auditing of each component.
- Require explainability: Avoid black-box systems where neither clinicians nor developers can trace why the chatbot said what it said. Explainable AI is an architectural choice, not an afterthought.
- Build AI literacy into the user experience: NAM recommends that platforms actively educate users about AI capabilities and limits. This should be a designed feature, not a buried disclaimer.
- Evaluate against clinical criteria: Use published CBT competency frameworks or standardized measures like the Cognitive Therapy Rating Scale to assess chatbot performance, not just user satisfaction scores.
- Plan for regulatory scrutiny: FDA advisory discussions are actively targeting generative AI mental health tools. Architecture decisions made today will face compliance review tomorrow.
Pro Tip: Before committing to any therapy chatbot platform, request documentation of its crisis escalation protocol. Test it yourself with simulated high-risk language. If the response is slow, generic, or absent, the architecture is not ready for clinical deployment.
Developers should also review therapy chatbot integration strategies to understand how leading platforms combine mental health assessments with conversational AI modules in practice.
Future trends and challenges in therapy chatbot architecture
The next generation of therapy chatbot architecture is moving in two directions simultaneously: greater capability and greater scrutiny.
| Trend | Opportunity | Challenge |
|---|---|---|
| Multimodal AI (voice, text, image) | Richer empathic understanding and more natural interaction | Increased complexity in safety monitoring and bias detection |
| Cognitive layer advancement | More precise therapeutic reasoning and personalized interventions | Requires ongoing clinical validation and model retraining |
| FDA and regulatory frameworks | Clearer standards for evidence, labeling, and crisis response | Compliance costs and potential market barriers for smaller developers |
| Cross-platform interoperability | Integration with EHR systems and clinical workflows | Data privacy, consent architecture, and security complexity |
| Explainable AI requirements | Greater clinician trust and auditability | Technical overhead and potential reduction in model flexibility |
FDA advisory committee discussions now explicitly address generative AI mental health tools, covering evidence standards, non-human labeling requirements, crisis response protocols, and clinical boundary definitions. Developers who treat these discussions as distant regulatory noise are making a strategic error.
User trust is the other major challenge. The impact of chatbot technology on therapy depends heavily on whether users understand what the system can and cannot do. Architecture that builds in transparency features, usage limit prompts, and regular check-ins with human clinicians will outperform systems that maximize engagement at the cost of appropriate boundaries.
My perspective on what architecture really means for therapy apps
I’ve spent considerable time examining how chatbot design in mental health has evolved, and the pattern I keep returning to is this: most failures in therapy app chatbots are not model failures. They are architecture failures.
I’ve seen platforms with genuinely impressive underlying models produce harmful interactions because there was no cognitive layer constraining the output to therapeutic principles. The model was capable. The architecture was not. That distinction matters enormously when you are working with people in genuine distress.
What I find most underappreciated is the trauma-informed design gap. Developers often treat TIC as a content concern, something to address in the copy or tone of voice guidelines. In reality, it is a structural requirement. The way a chatbot manages silence, pacing, user control, and escalation must be built into the architecture itself. You cannot write your way out of a bad system design.
My honest advice to mental health professionals evaluating platforms: stop asking “what AI does it use?” and start asking “how is the AI constrained?” The answer to the second question tells you far more about whether the system is safe for your clients.
For developers, the collaboration imperative is real. The best therapy chatbot architectures I have encountered were built by teams where clinicians had genuine veto power over design decisions, not just advisory roles. That is not a process preference. It is a safety requirement.
— dushyantha
How Cognicareai supports smarter therapy chatbot development
If you are building or evaluating therapy chatbots and want to understand which platforms actually implement the architectural principles covered in this article, Cognicareai is a strong starting point.
Cognicareai curates a directory of AI-powered mental health tools with a focus on clinical effectiveness, safety protocols, and evidence-based design. Rather than pointing you toward the most marketed platforms, it surfaces tools that have demonstrated real therapeutic value. Whether you are a developer researching architecture patterns or a clinician assessing digital health options for your practice, the Cognicareai mental health AI directory gives you a structured way to compare tools against the criteria that actually matter. You can also explore the top AI-powered mental health tools reviewed for clinical design quality and safety architecture.
FAQ
What is chatbot architecture in therapy apps?
Chatbot architecture in therapy apps refers to the full technical and clinical structure of a conversational AI system, including its language model, cognitive reasoning layer, assessment modules, crisis escalation protocols, and security design. It determines how the chatbot behaves therapeutically, not just conversationally.
Can a therapy chatbot outperform a human therapist?
On specific CBT competency measures, yes. A cognitive layer architecture outperformed both standalone LLMs and human clinicians in a randomized trial, though this applies to structured competency tasks rather than the full scope of human therapeutic relationships.
What safety features should a therapy chatbot architecture include?
At minimum, a therapy chatbot should include automated crisis detection, emergency escalation to human support, session monitoring and audit logging, and clear non-human disclosure. Safety escalation protocols become more critical as the underlying model becomes more flexible.
How do trauma-informed care principles apply to chatbot design?
SAMHSA’s six TIC principles, including safety, transparency, and cultural sensitivity, must be embedded as architectural features rather than content guidelines. A scoping review of 28 mental health chatbots found most existing platforms fall short on TIC compliance.
What regulatory requirements apply to therapy chatbots in 2026?
FDA advisory committees are actively evaluating generative AI mental health tools, with discussions covering evidence standards, non-human labeling, crisis response requirements, and clinical boundary definitions. Developers should treat FDA digital health guidance as an active compliance concern, not a future consideration.